
Sangeeta Das* and Pankaj Deka
Department of Veterinary Microbiology, CVSc, AAU, Khanapara
*Email: sangeetadas31280@gmail.com
International Encyclopedia of Public Health defines “disease eradication” as the status of‘global zero disease due to control measures which are no longer required’. Efforts to eradicate infectious diseases began with the programme of eradication of hookworm and yellow fever initiated in the early 1900s, yaws in the 1940s, and malaria in the 1950s. Despite failure in the eradication programmes, valuable lessons were learned, and new ways were invented to tackle them. Louis Pasteur quoted that “it is within the power of man to eradicate infection from the earth” and this power has so far made possible eradication of smallpox in humans and rinderpest (cattle plague) in animals. The possibility became apparent with the invention of the first vaccine against smallpox by Edward Jenner in 1796. It took almost 200 years to eradicate the disease. The last recorded case of smallpox occurred in 1977 in Somalia and the disease was officially declared eradicated by the World Health Organization (WHO) in 1980. Since the global eradication of smallpox, there has been widespread interest on infectious disease eradication as a public health goal. Eradication efforts for rinderpest, the only animal disease successfully eradicated so far, began in 1920s before a vaccine was available against the disease by adopting measures such as animal quarantine and slaughter. In 1960, a vaccine against rinderpest was developed by Walter Plowright which finally led to its eradication. The last case was recorded in Mauritania in 2003 and in 2011, the World Organization for Animal Health (OIE) declared rinderpest as eradicated globally. The process of disease eradication is always a very long. It not only depends on scientific contexts but political and bureaucratic frameworks also to support feasible measures such as vaccination efforts, health campaigns etc. for successful eradication.

Fig: Smallpox blisters on arm
Source: https://www.flickr.com/photos/99129398@N00/3508802522
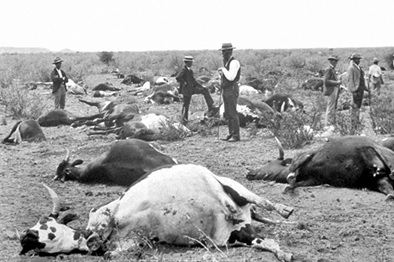
Fig: Cattles died due to rinderpest in South Africa, 1896
Source: https://upload.wikimedia.org/wikipedia/commons/3/36/Rinderpest_1896-CN.jpg
The key concept to infectious disease eradication involves three words that are commonly used interchangeably: control, elimination and eradication. By control, we mean intervention that interrupts the circulation and/ or transmission of an infectious agent from the local perspective. Like control, elimination is also location-specific and requires interventions to prevent re-emergence of the disease. In contrast, eradication is permanent and global. It means zero disease or total absence of any cases, the absence of a reservoir for the infectious agent and absolute containment of any infectious source. There is no defined path for eradication rather it entails risk. The conquer of smallpox and rinderpest,improvement and advances in surveillance, diagnostics, therapeutics, and vaccines with an associated health system infrastructure, raised hopes that infectious diseases are conquerable. The International Task Force for Disease Eradication (ITFDE) that advises bodies such as the WHO on different aspects of disease eradication, listed polio and dracunculiasis (Guinea worm disease) as potentially eradicable whereas mumps, measles, rubella, lymphatic filariasis and cysticercosis could only be eliminated from some parts of the world.
Control measures have led to tremendous reduction in the incidence of infectious diseases affecting human and animal health. Mass vaccination campaigns have interrupted circulation of poliomyelitis, measles and rubella in humans and have reduced the incidence of foot and mouth disease (FMD), brucellosis and canine rabies in animals. Mass drug administration has significantly reduced the infection intensity of lymphatic filariasis, onchocerciasis and dracunculiasis. So, what makes a disease eradicable? Most importantly, an eradicable disease should be infectious, should have a major host, effective treatments or vaccines should be available for the disease and there should be political and/ or financial support for the eradication efforts. The disease aspects that make eradication likely are:
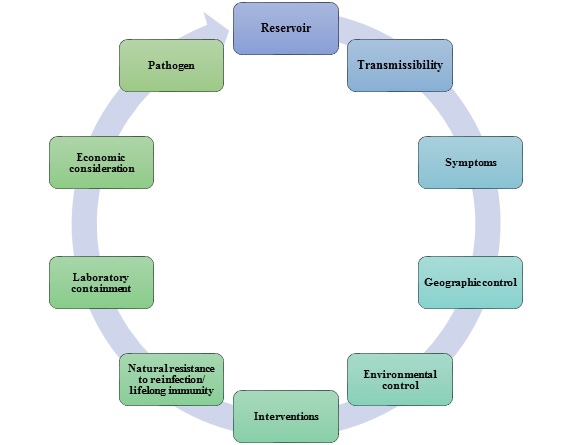
Fig: Disease aspects that make eradication likely
- Pathogen: A disease caused by multiple pathogens is difficult to eradicate. Variola virus, the causative agent of smallpox only infects human and human-to-human transmission could be interrupted through vaccination. In contrast, the economically important disease of livestock, FMD, is difficult to eradicate due to the existence of multiple serotypes of the FMD virus.
- Reservoir: Disease causing pathogens may infect multiple species or may exist in a species that serves as a reservoir or a vector for transmission. Even if the diseases are eliminated in the host population, the existence of the pathogen in non-human reservoirs or vectors allows reinfection. The presence of an animal reservoir (non-human primate) hampered eradication of yellow fever. Therefore, a disease with multiple hosts is difficult to be targeted for eradication. For example, eradicating African swine fever (ASF) is highly complex due to the maintenance of ASF virus in wild boars and multiple species of soft tick (Ornithodoros) However, a disease caused by a single-host pathogen (polio, measles, Guinea worm disease etc.) may also present additional challenges.
- Transmissibility: For a disease to be controlled, its transmission has to be stopped. It depends on the reproduction number (R0) that measures the transmission potential of a disease and must be maintained at below 1.0. It is influenced by several factors such as population density of the vectors, and/ or intermediary hosts, environmental conditions etc.
- Symptoms: For successful eradication, a disease should be easily diagnosable or recognizable. The smallpox eradication campaign got benefitted from the characteristic symptoms that allowed health officials worldwide to diagnose the infection easily. Some diseases are not detectable due to the latent infections (such as Tuberculosis) (https://www.cdc.gov/tb/worldtbday/history.htm) whereas some diseases may limit the ability to treat them when symptoms may be visible (Hepatitis C).Likewise, in pigs, ASF and classical swine fever (CSF) are clinically similar and cannot be definitively distinguished from each other in the field. For a disease to be favorable for eradication, it should have a highly characteristic syndrome, an easy and a reliable diagnostic tool with high sensitivity and specificity.
- Geographic control: The global community is affected by many diseases. As a disease becomes more geographically restricted, targeted campaigns prove beneficial to push the disease to the brink of eradication.
- Environmental control: The ecological niche of microbial pathogens is determined by the environmental variations, intermediary vectors and hosts in complex biological systems. Moreover, some infectious agents have a longer latency period and are highly transmissible (measles, rubella, influenza, FMD, ASF and CSF) that are driven by seasonal environmental factors and population-based immunity, indicating a global pattern of distribution.
- Interventions: Vaccination had a striking impact on eradication strategies as an effective intervention to interrupt transmission of the agent. The smallpox and the rinderpest eradication strategies as well as most of the ongoing disease elimination campaigns rely on vaccines. Recently, the Hon’ble Prime Minister of India launched a flagship scheme – “National Animal Disease Control Programme (NADCP)” in September 2019 for control of FMD and brucellosis in the country by vaccinating 100% of cattle, buffalo, sheep, goat, and pig populations for FMD and 100% of bovine female calves aged 4-8 months for brucellosis with a total financial outlay of Rs. 13,343.00 crores for five years (2019-20 to 2023-24) (https://dahd.nic.in/schemes/programmes/nadcp). The government is also focusing on vaccination of livestock against another emerging disease– lumpy skin disease (LSD) (https://timesofindia.indiatimes.com/india/centre-states-trying-to-control-spread-of-lumpy-skin disease-in-cattle-pm-modi/articleshow/). The important factor favoring disease eradication by vaccination include availability of a highly effective, safe, cheap and stable vaccine with long-lastingimmunity. Besides, other interventions such as the “Information Network for Animal Productivity and Health (INAPH)”, also known as “Pashu Aadhaar” has also been developed where digital or biometric identification of livestock is being done to keep track of their population and health (https://www.business-standard.com/article/current-affairs/pashu-aadhaar-how-will-it-help-control-lumpy-skin-disease-in-cattle).
- Natural resistance to reinfection/ lifelong immunity: Reducing the susceptible populations in endemic areas by inducing long-lasting immunity through vaccination or natural infections is important for a successful disease eradication programme.
- Laboratory containment: A satisfactory containment and maximum security of specimens containing the targeted organisms is necessary for eradication in laboratories, as they could also serve as reservoirs.
- Economic consideration: The initial costs of disease eradication efforts are very high, and it may take many years to achieve. It not only depends on scientific contexts but also on the estimated cost of eradication and political stability of the affected countries. The Global Polio Eradication Initiative (1988) illustrated the effort from international to national and community levels that reduced the number of paralytic polio cases with only three countries endemic today (Pakistan, Afghanistan, and Nigeria). The costs and benefits of global eradication programmes can have direct or consequent effects. The direct effects are that no morbidity or mortality will ever again occur whereas the consequent effects are those that impact either positively or negatively on the entire health facility. From the economic perspective, a disease is not always global but may be found only in poor tropical countries demanding international financing.
The success of eradication has so far been limited only to one human and one animal disease for several reasons. The first important reason is the function of the biology of the specific pathogen involved. Second, being host-specific, these diseases had no reservoir to hide. Equally important is the development of lifelong immunity against infection. Therefore, the eradication strategy should lie on a long-term preventive vision rather than a short-term curative domain of action with the potential to effectively respond to the evolution of unwanted epidemiological traits such as resistance to antimicrobials and insecticides. The defeat of Global Malaria Eradication Programme (1955-69) was due to development of drug resistance among the pathogen and resistance of mosquito vectors to insecticides. It requires large-scale pilot programmes ahead of eradication effort, global coordination, and surveillance of the disease outbreaks at the international level, and maintenance of public trust in science and global health initiatives. To extend the life span of disease prevention strategies, future research should explore multiple dimensions involving host-pathogen interaction, environmental parameters, and evolutionary thinking with sustainable solutions. For example: dracunculiasis or Guinea worm disease, the first parasitic disease targeted for eradication could not be controlled alone by vaccination, as there exist no effective vaccines or therapeutics. It is here where creative disease containment strategies come into play for discovering transmission-disrupting alternatives that do not rely on having a vaccine. As it is caused by ingestion of contaminated water, community education, provision of non-contaminated water and active surveillance may help in reducing the disease incidence. Presently, WOAH and its partners have undertaken eradication strategy for a few animal diseases namely, ASF, bovine tuberculosis, FMD, Peste des petits ruminants (PPR) and rabies (https://www.woah.org/en/what-we-do/global-initiatives/disease-eradication/).
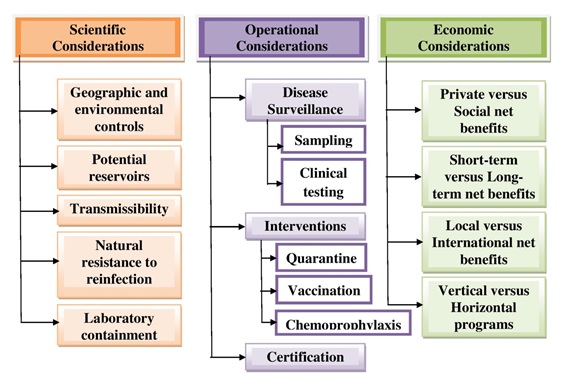
Fig: The framework for infectious disease eradication
The smallpox and the rinderpest success stories have been inspirational that made eradication programme a steady progress by planning extended control measures. However, can the world eradicate another disease? The final outcome of a disease eradication programme may be uncertain but the effort will always be worth taking. Even if we cannot eradicate all the infectious diseases, we may be able to keep them at bay with sustainable solutions. With continued efforts and changes in perspectives, the goals which are not yet feasible could now be achieved, and the world can hope to eradicate another important infectious disease in the near future.
References:
Biswas, G.; Sankara, D.P.; Agua-Agum, J. and Maiga, A. (2013). Dracunculiasis (guinea worm disease): eradication without a drug or a vaccine. Philosophical Transactions of the Royal Society B. 368: 20120146. doi:10.1098/rstb.2012.0146.
Das, S.; Deka, P.; Deka, P.et al. (2021). African swine fever: Etiology, epidemiology, control strategies and progress toward vaccine development: A comprehensive review. Journal of Entomology and Zoology Studies. 9(1): 919-929.
Dubos, R. and Dubos, J. (1953). The White Plague: Tuberculosis, Man and Society. London: Gollancz. Quoted in Fenner, Hall, and Dowdle, 1998.
Feachem, R.G.A.; Chen, I.; Akbari, O. et al. (2019). Malaria eradication within a generation: ambitious, achievable, and necessary. Lancet. 394(10203): 1056-1112. doi:10.1016/S0140-6736(19)31139-0.
Fenner, F.; Henderson, D.A.; Arita, I.; Ježek, Z. and Ladnyi, I.D. (1988). Smallpox and Its Eradication. Geneva: World Health Organization.
Henderson, D.A. (1999). Lessons from the eradication campaigns. Vaccine. 17: S53–S55.doi:10.1016/S0264-410X(99)00293-5.
Jacobson, J. (2011). The role of research. Disease eradication in 21st century. Cambridge, MA: MIT Press.
Jeffrey, G.M. (1976). Malaria Control in the Twentieth Century. American Journal of Tropical Medicine and Hygiene. 25: 361–71.
Jenner, E. (1801). The Origin of Vaccine Inoculation. London: Shury. Quoted in Fenner, Hall, and Dowdle, 1998.
Nájera, J.A.; González-Silva, M. and Alonso, P.L. (2011). Some lessons for the future from the Global Malaria Eradication Programme (1955–1969). PLoS Medicine. 8: e1000412. doi:10.1371/journal.pmed.1000412.
NCDC (2023). National Centre for Disease Control, Directorate General of Health Services, Ministry of Health & Family Welfare, Government of India (https://ncdc.mohfw.gov.in/).
Newby, G.; Mpanju-Shumbusho, W. and Feachem, R.G.A. (2021). Global health security requires endemic disease eradication. Lancet. 397(10280): 1163-1165. doi:10.1016/S0140-6736(21)00521-3.
Sumption, K.; Domenech, J. and Ferrari, G. (2012). Progressive control of FMD on global scale. Veterinary Record. 170: 637–639. doi:10.1136/vr.e4180.
WHO (2021). WHO Collaborating Center for Dracunculiasis Eradication, Guinea Worm Wrap-Up #283, Centers for Disease Control and Prevention (CGH): Atlanta.
*************************************



{kind=link}